
Bloodborne pathogen exposure risk is a serious issue for healthcare workers who handle blood and body fluids. It can spread through needlesticks, cuts, or direct contact with infected blood. Diseases like hepatitis and HIV are major concerns in such situations. Using proper protective equipment and following safety protocols helps reduce the risk and keep workers safe.
What “Most Common Risk Actually Means in This Context
The most common risk of exposure to bloodborne pathogens for healthcare workers is percutaneous injury specifically needlestick injury in which a contaminated needle or sharp object punctures the skin and delivers infected blood directly into the body. This route accounts for the vast majority of occupational bloodborne pathogen transmissions in healthcare settings.
The major source of bloodborne infections in healthcare settings is via percutaneous injuries from needles or other sharps. Other exposure routes exist mucous membrane splashes, non-intact skin contact, human bites but none come close in frequency or transmission risk.
Why Needlestick Injuries Dominate: The Biology Behind the Risk
Needlestick injuries are one of the most significant concerns in healthcare settings because they provide a direct pathway for bloodborne pathogens to enter the body. Unlike surface contact, these injuries bypass the skin’s natural protective barrier, allowing viruses and bacteria present in contaminated blood to reach the bloodstream instantly. This makes even a tiny puncture potentially dangerous, especially when dealing with infectious patients or used medical sharps.
Direct Blood-to-Blood Transmission Pathway
The main biological reason needlestick injuries are so dangerous is that they create a direct route for infected blood to enter another person’s circulatory system. Viruses like Hepatitis B, Hepatitis C, and HIV thrive in blood, and even a microscopic amount transferred through a needle can carry enough viral load to cause infection. Since needles are designed to penetrate tissue, they efficiently bypass external defenses like skin, making transmission highly efficient compared to other exposure types.
High Viral Stability and Sharp Contamination Risk
Many bloodborne pathogens can survive on medical instruments for extended periods, especially in unsterilized conditions. Used needles may retain infectious material on both the surface and inside the hollow bore, increasing the risk of exposure during accidental pricks. In fast-paced healthcare environments, improper disposal, recapping needles, or emergency procedures can further elevate the chances of injury, making strict safety protocols essential to minimize risk.
Which Healthcare Workers Face the Highest Risk By Role
Among physicians, surgeons are the group at highest risk for needlestick exposure, with surgical residents representing the subgroup at highest risk overall.The combination of long procedures, fatigue, confined surgical fields, and high needle density makes the operating room the single most dangerous environment for percutaneous injury.
Among all healthcare workers, nurses account for 24% of reported HIV exposure cases a figure that reflects their sheer volume of needle-dependent procedures: IV placements, blood draws, medication administration, and post-procedure cleanup.
Phlebotomists, ICU nurses, and emergency department staff round out the high-exposure roles. The CDC estimates approximately 18 million workers in the healthcare industry are at risk for occupational exposure to bloodborne pathogens.
Quick Comparison Exposure Risk by Healthcare Role:
| Role | Primary Risk Scenario | Key Exposure Moment | Risk Level |
| Surgical resident | Intraoperative needle handling | Suturing under time pressure | Highest |
| ICU nurse | IV line management, blood draws | Disposal and recapping | High |
| Phlebotomist | Venipuncture (high volume) | Post-draw needle removal | High |
| Emergency RN | Trauma procedures, unknown source patients | Rapid IV access, chaotic environments | High |
| Medical assistant | Injections, specimen handling | Recapping, disposal | Moderate–High |
When Needlestick Injuries Happen: The Three Danger Windows
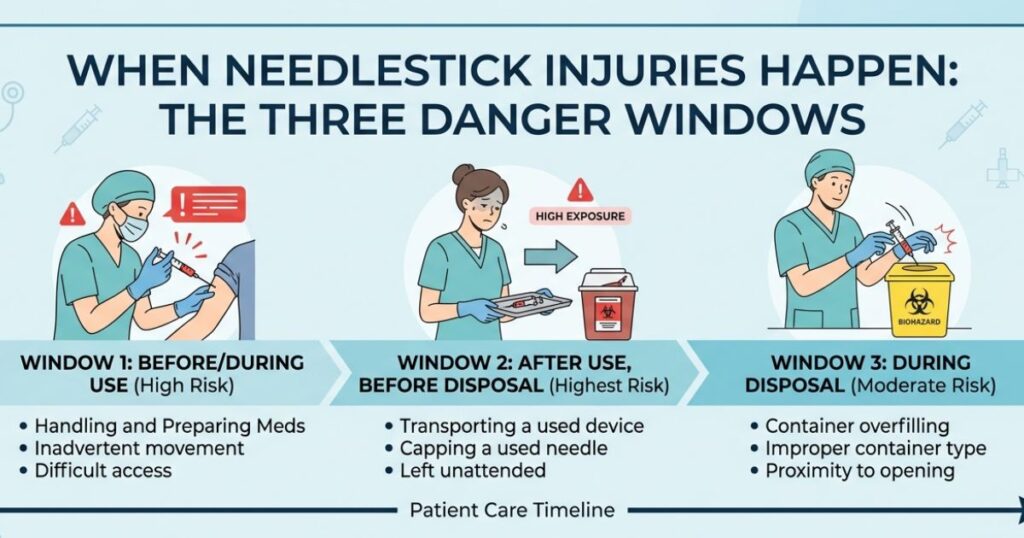
Needlestick injuries are serious occupational hazards, especially for healthcare workers who handle needles and sharp instruments daily. These injuries can expose a person to bloodborne pathogens such as hepatitis B, hepatitis C, and HIV. Understanding the “three danger windows” after a needlestick injury is crucial for taking immediate action, reducing infection risk, and ensuring proper medical care. Quick response and correct steps can make a major difference in preventing long-term health complications.
Immediate Exposure Window (First Few Seconds to Minutes)
The first and most critical danger window occurs immediately after the injury. At this stage, blood or contaminated fluid enters the skin through the puncture wound. The priority is to act fast—wash the area thoroughly with soap and running water, avoid squeezing the wound, and report the incident immediately. Early response can significantly reduce the risk of infection.
Post-Exposure Window (First 24 to 72 Hours)
The second window is the post-exposure period, where medical evaluation becomes essential. During this time, healthcare professionals may recommend baseline blood tests, risk assessment of the source patient, and possibly post-exposure prophylaxis (PEP) for infections like HIV. Timely treatment within this window is highly effective in preventing disease transmission.
The Tools That Have Changed the Risk Landscape
The Needlestick Safety and Prevention Act (2000) fundamentally reshaped hospital protocol. Promotion of safety needles and needleless devices, along with other interventions, has resulted in a significant decline in percutaneous injuries among healthcare workers in the U.S.
BD (Becton, Dickinson and Company) is the dominant manufacturer of safety-engineered sharps devices retractable needles, passive safety syringes, and needleless IV connectors now standard in most U.S. hospital systems. Their SafetyGlide and Vacutainer Eclipse products represent the engineering controls OSHA mandates employers to consider under 29 CFR 1910.1030.
What to Do Immediately After a Needlestick Exposure
A needlestick injury is a medical emergency that requires fast and correct action to reduce the risk of infection from bloodborne diseases like hepatitis B, hepatitis C, and HIV. The steps taken in the first few minutes are very important and can greatly lower the chance of complications. Staying calm and following proper safety procedures helps ensure the best possible outcome after exposure.
Step 1: Clean the Injury Area Right Away
As soon as the injury happens, wash the affected area thoroughly with soap and running water. Do not squeeze or scrub the wound aggressively, as this may worsen tissue damage. If soap and water are not available immediately, use an antiseptic solution, but proper washing should still be done as soon as possible.
Step 2: Report and Seek Medical Attention
After cleaning the wound, report the incident to a supervisor or infection control department immediately. Seek medical evaluation without delay so that risk assessment and necessary tests can be done. In some cases, post-exposure prophylaxis (PEP) may be started quickly to reduce the risk of infection.
Conclusion
Bloodborne pathogen exposure remains a serious occupational hazard for healthcare workers, especially in high-risk settings such as emergency care, surgery, and laboratories. However, most exposures are preventable through strict adherence to safety protocols, proper use of personal protective equipment (PPE), safe handling of sharps, and timely reporting of incidents. Continuous training and awareness play a vital role in reducing infection risks and ensuring a safer healthcare environment for both staff and patients.
FAQs
What’s the most common bloodborne pathogen transmitted through needlestick injuries?
Hepatitis B (HBV) is the most efficiently transmitted bloodborne pathogen via needlestick, with transmission risk up to 31% in high-infectivity scenarios. HCV and HIV also transmit this way but at lower rates.
How do I know if a needlestick injury is serious enough to report?
Report every needlestick, regardless of how minor it seems. The source patient’s infection status, needle type, and depth of injury all affect risk and you can’t assess those factors yourself in the moment.
Should I get the hepatitis B vaccine before starting a clinical role?
Yes complete the three-dose HBV series before patient contact if possible. An unvaccinated worker faces up to 31% transmission risk from a single needlestick with a high-infectivity source.
Why does recapping needles cause so many injuries?
Two-handed recapping forces the non-dominant hand into the path of the needle tip. Even a small hand tremor or moment of distraction results in puncture. One-handed or mechanical recapping eliminates this entirely.
When should I call PEPline after a needlestick?
Immediately or within two hours at the absolute latest for HIV post-exposure prophylaxis eligibility. Don’t wait for occupational health to open the next morning.